









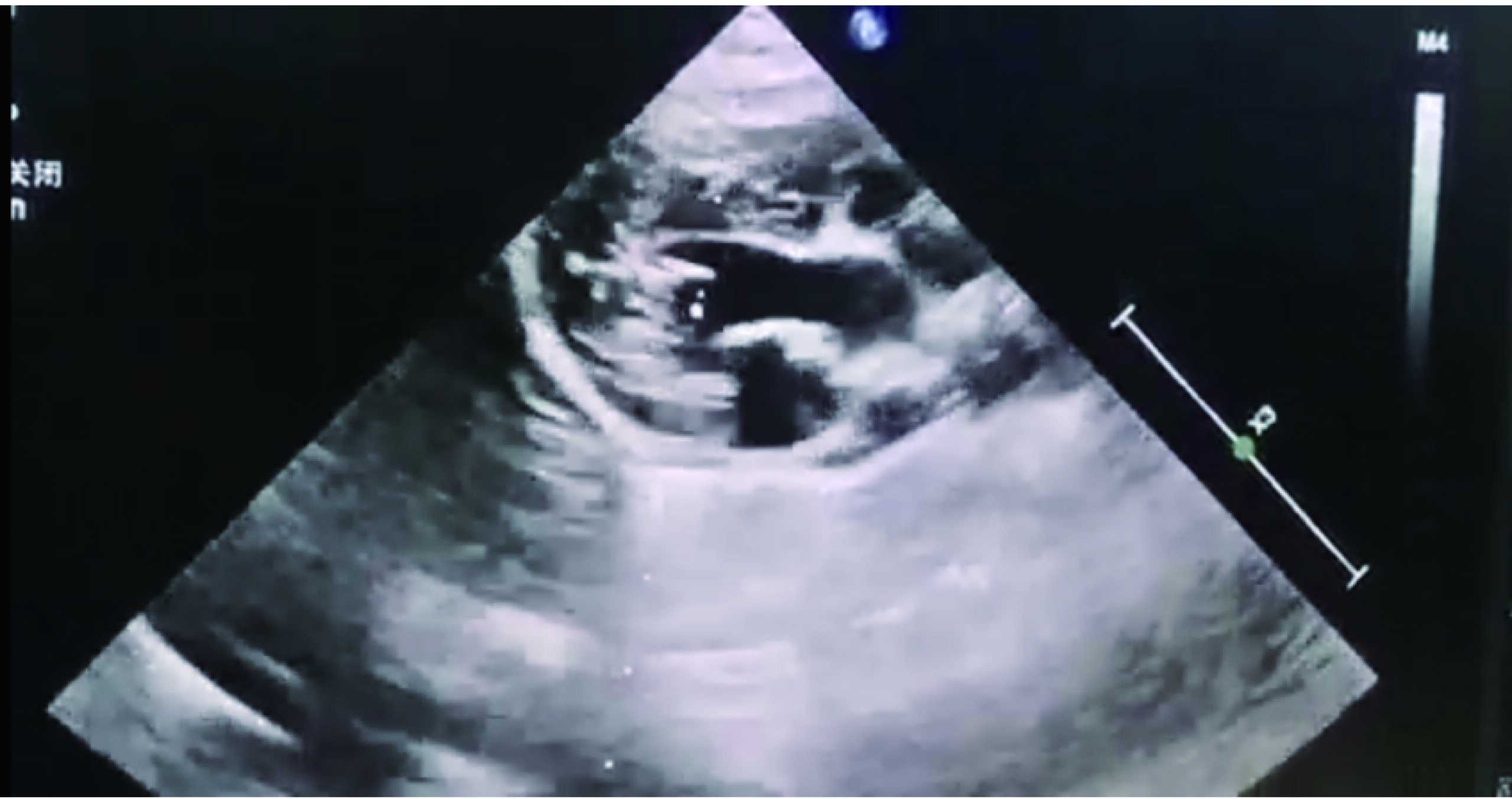
Figure 1
Left ventricular long-axis view in hypertensive heart disease
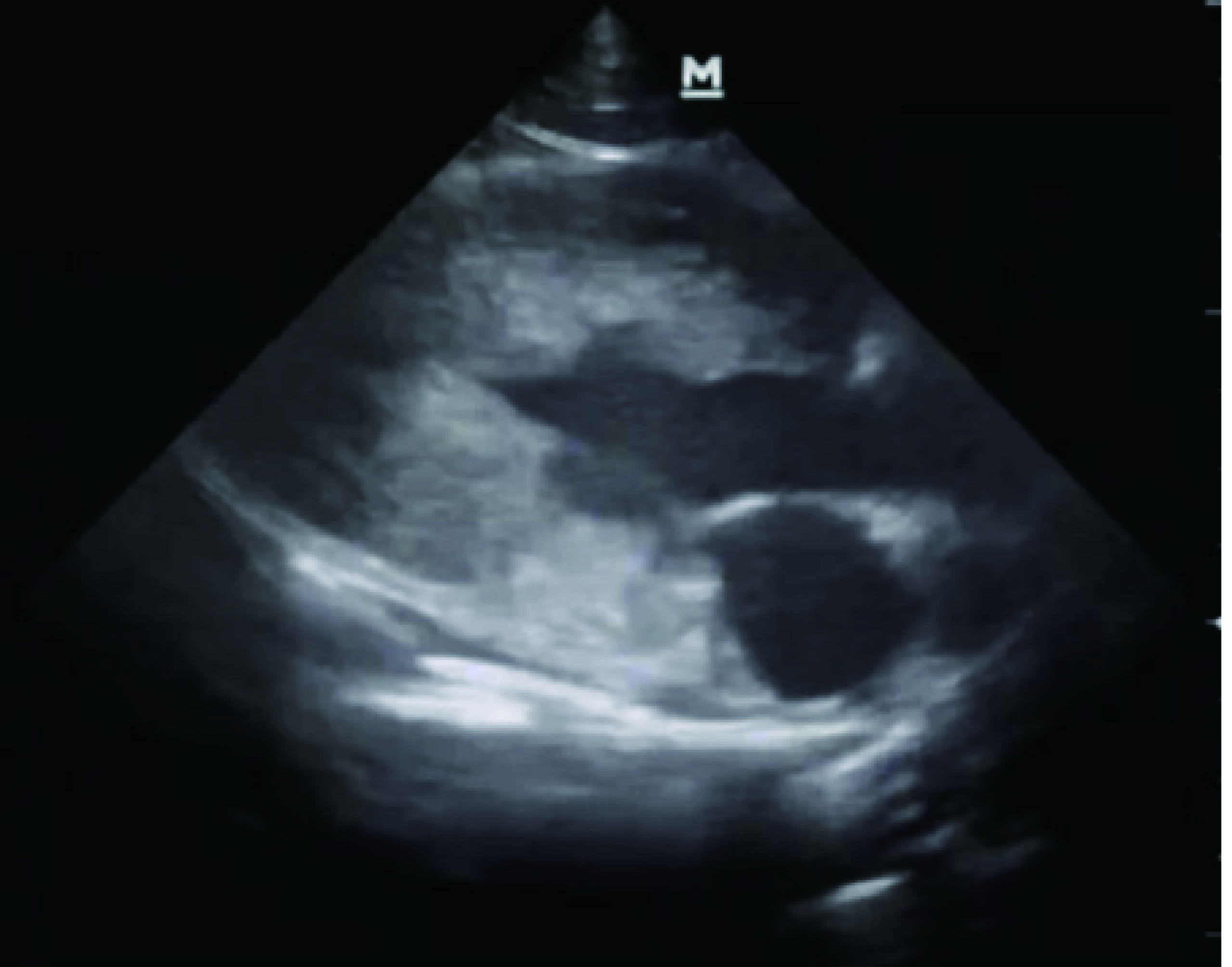
Figure 2
Left ventricular long-axis view in hypertrophic cardiomyopathy
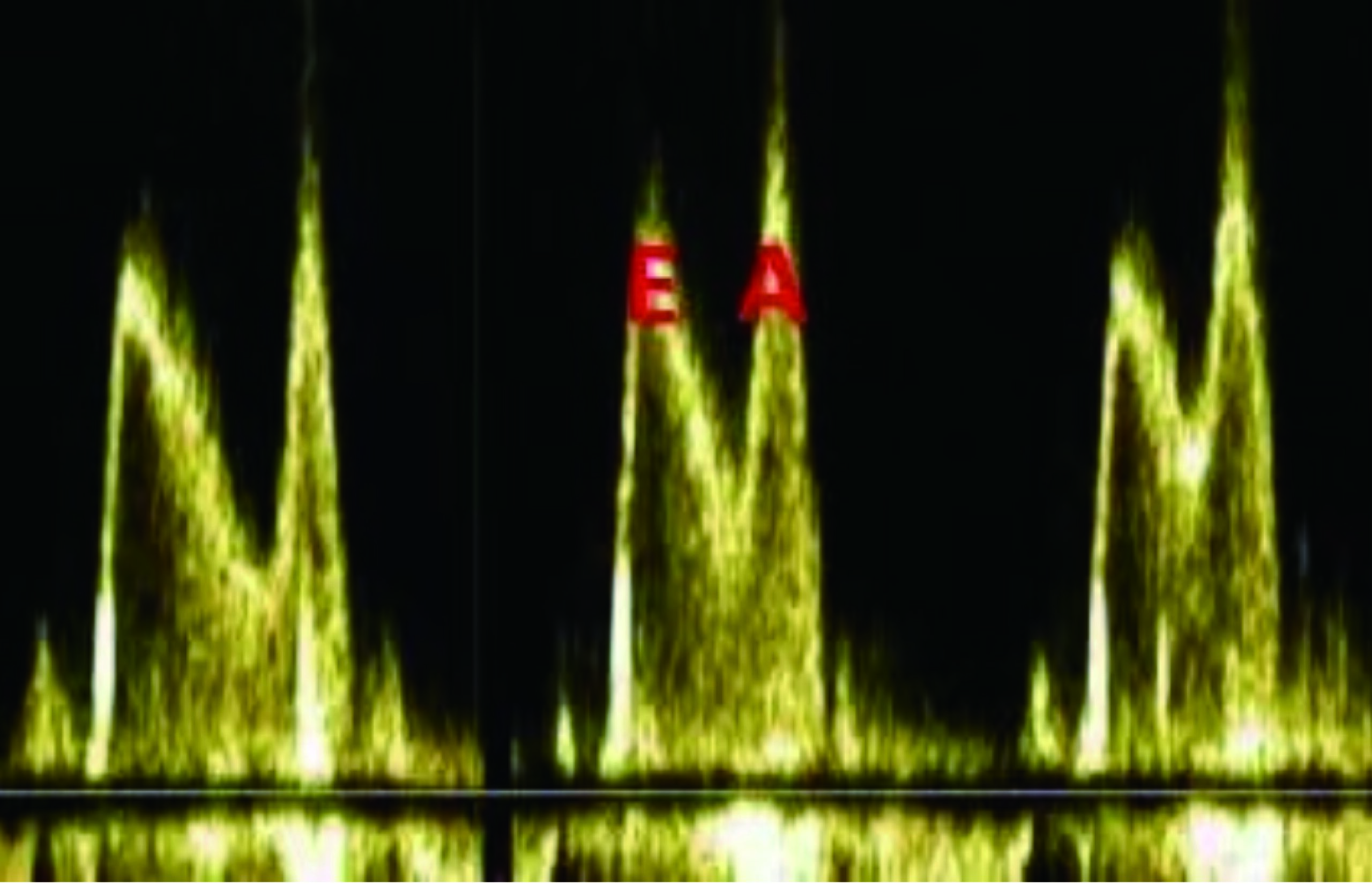
Figure 3
E/A ratio <1
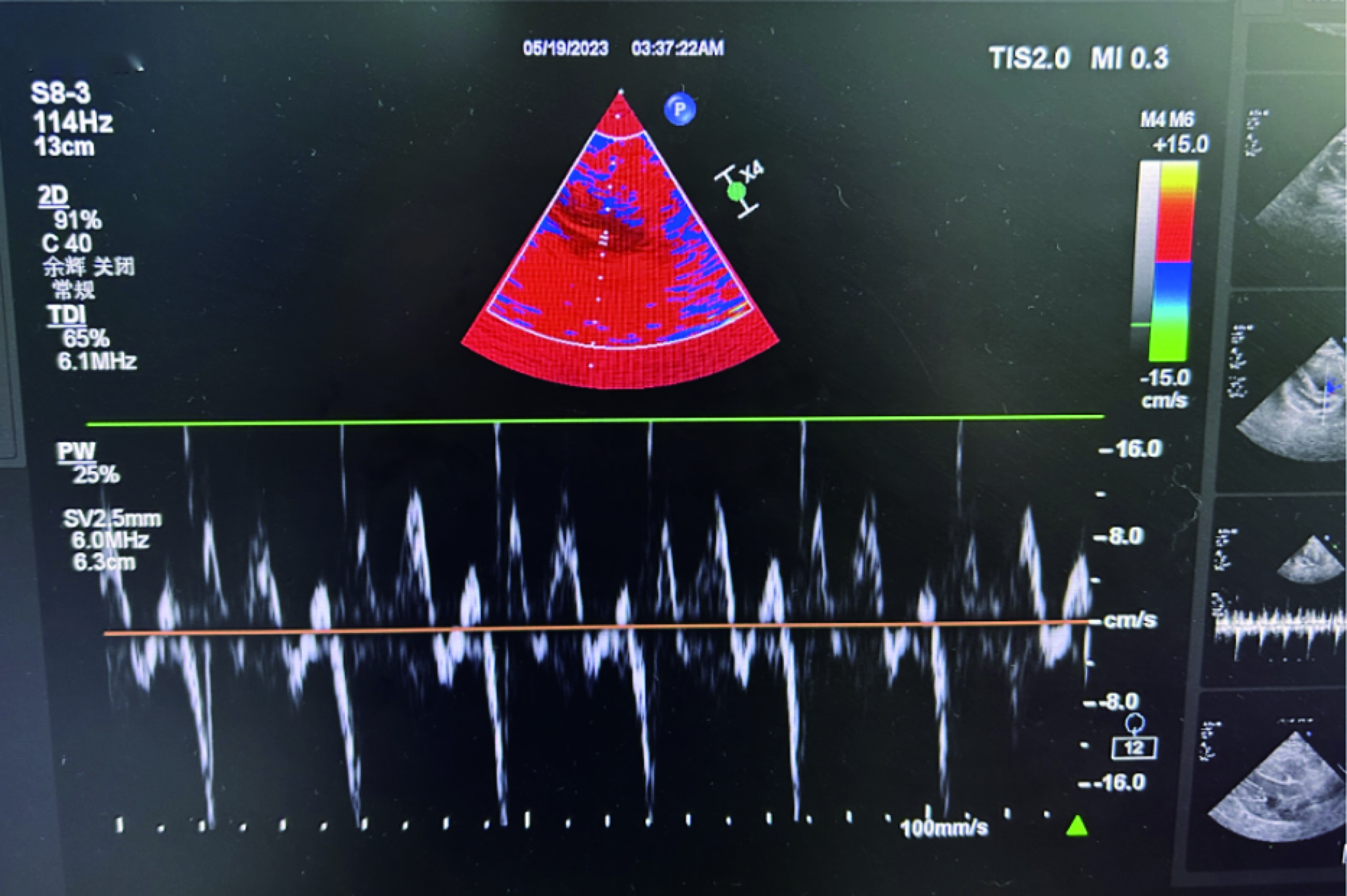
Figure 4
Tissue Doppler imaging (TDI) showing e'/a' ratio <1
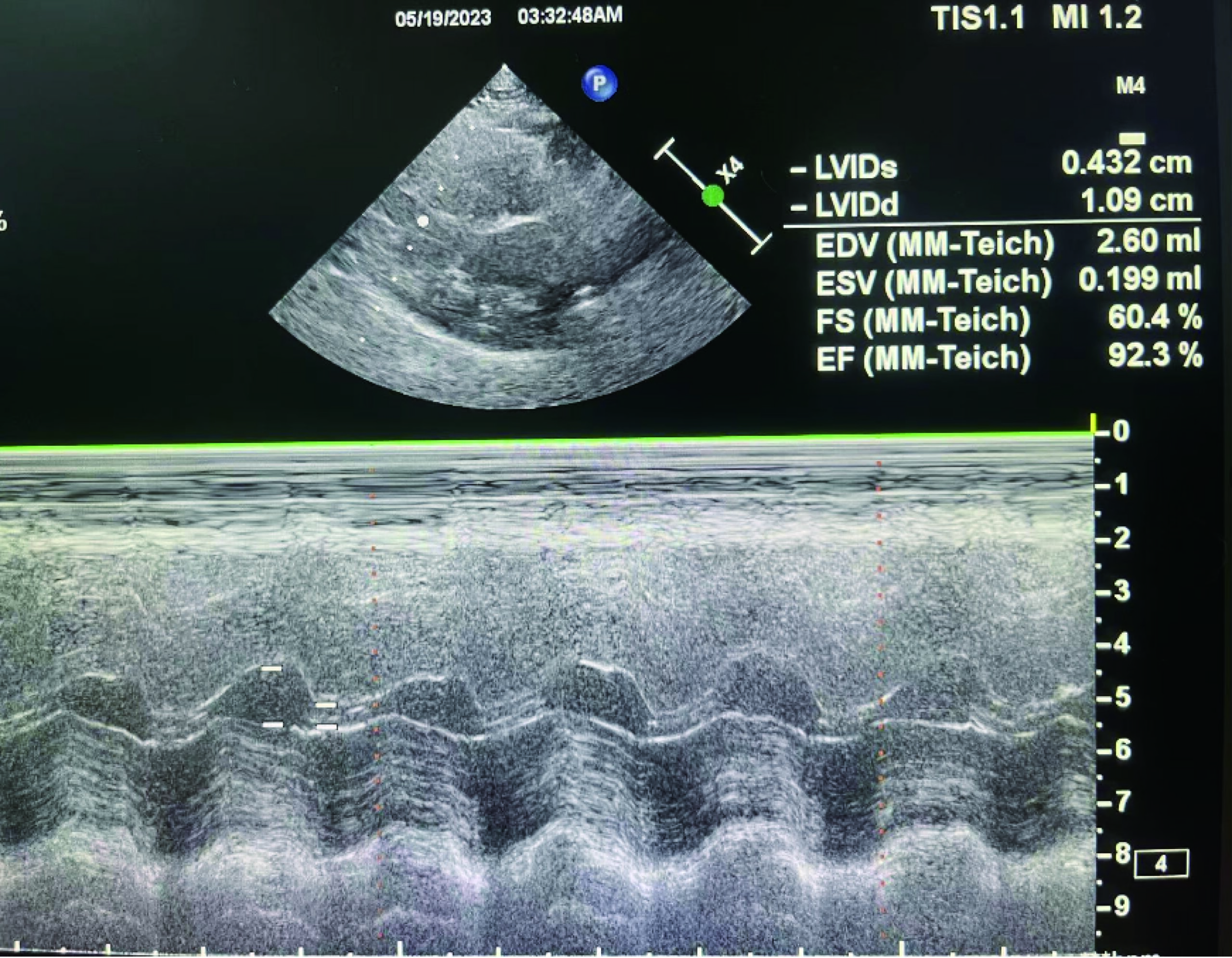
Figure 5
EF >92% (measured via MM-Teich method)

Figure 6
Atrial fibrillation