









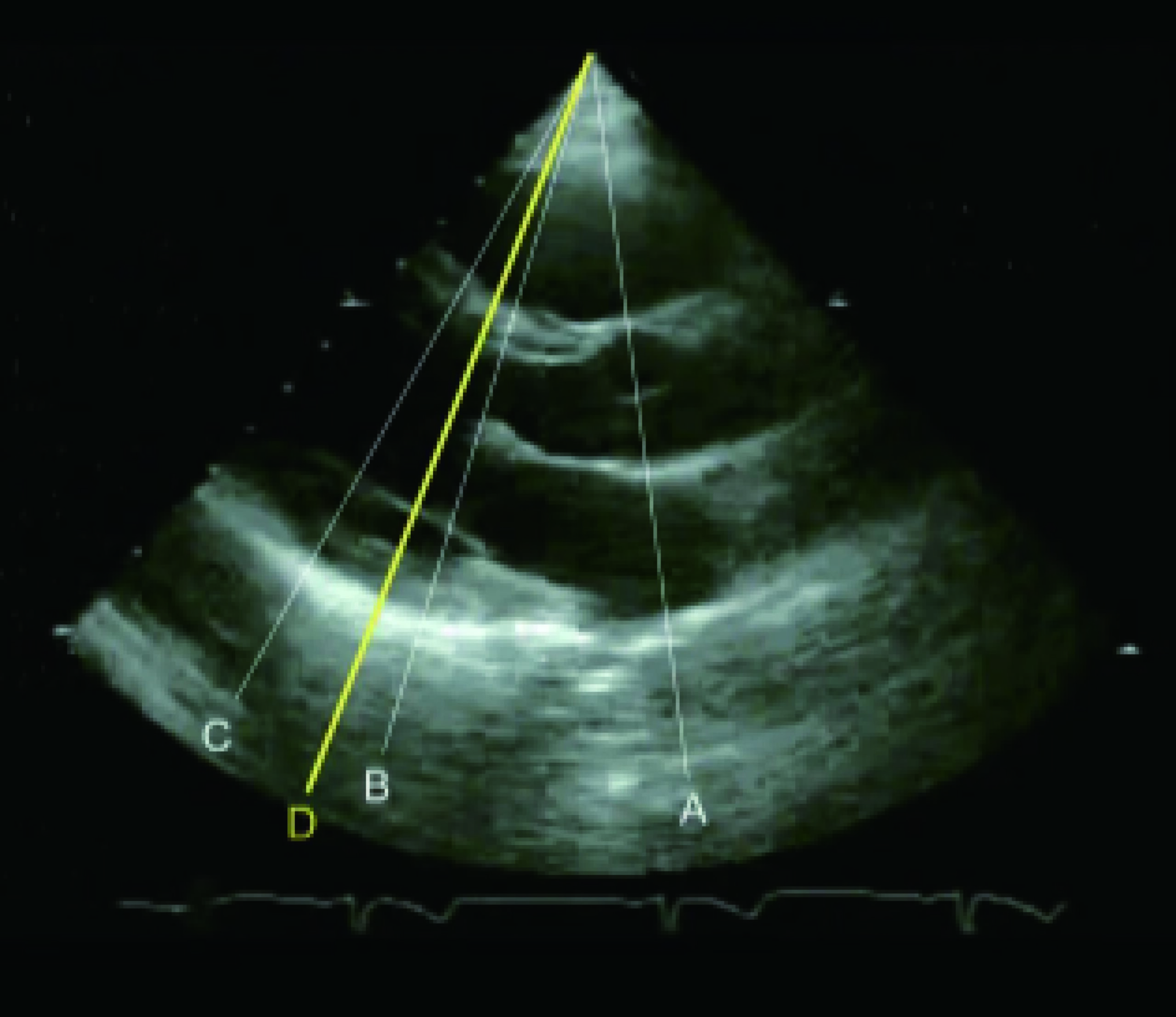
Figure 1
Left ventricular long-axis view (Groups A, B, C)
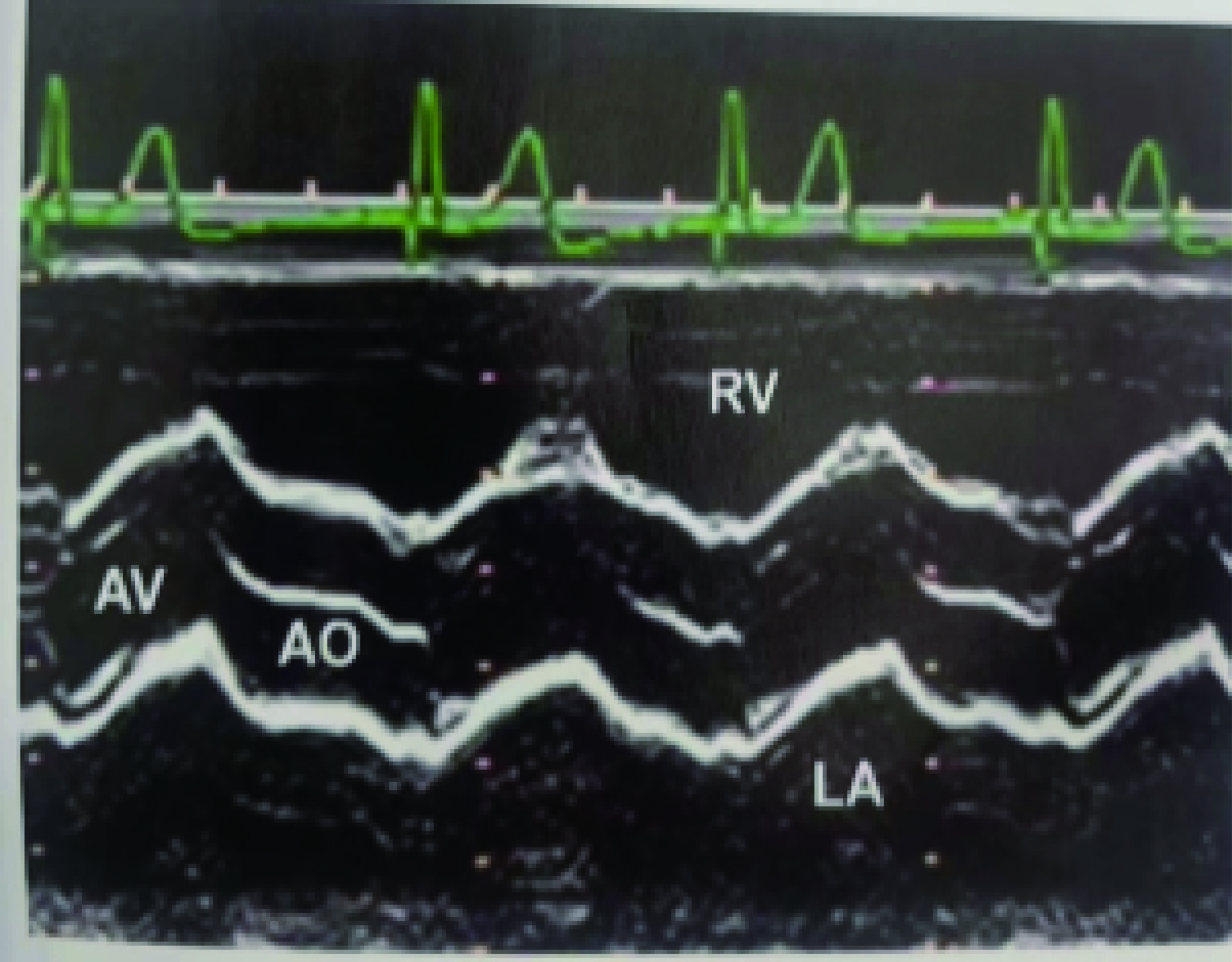
Figure 2
Aortic root waveform
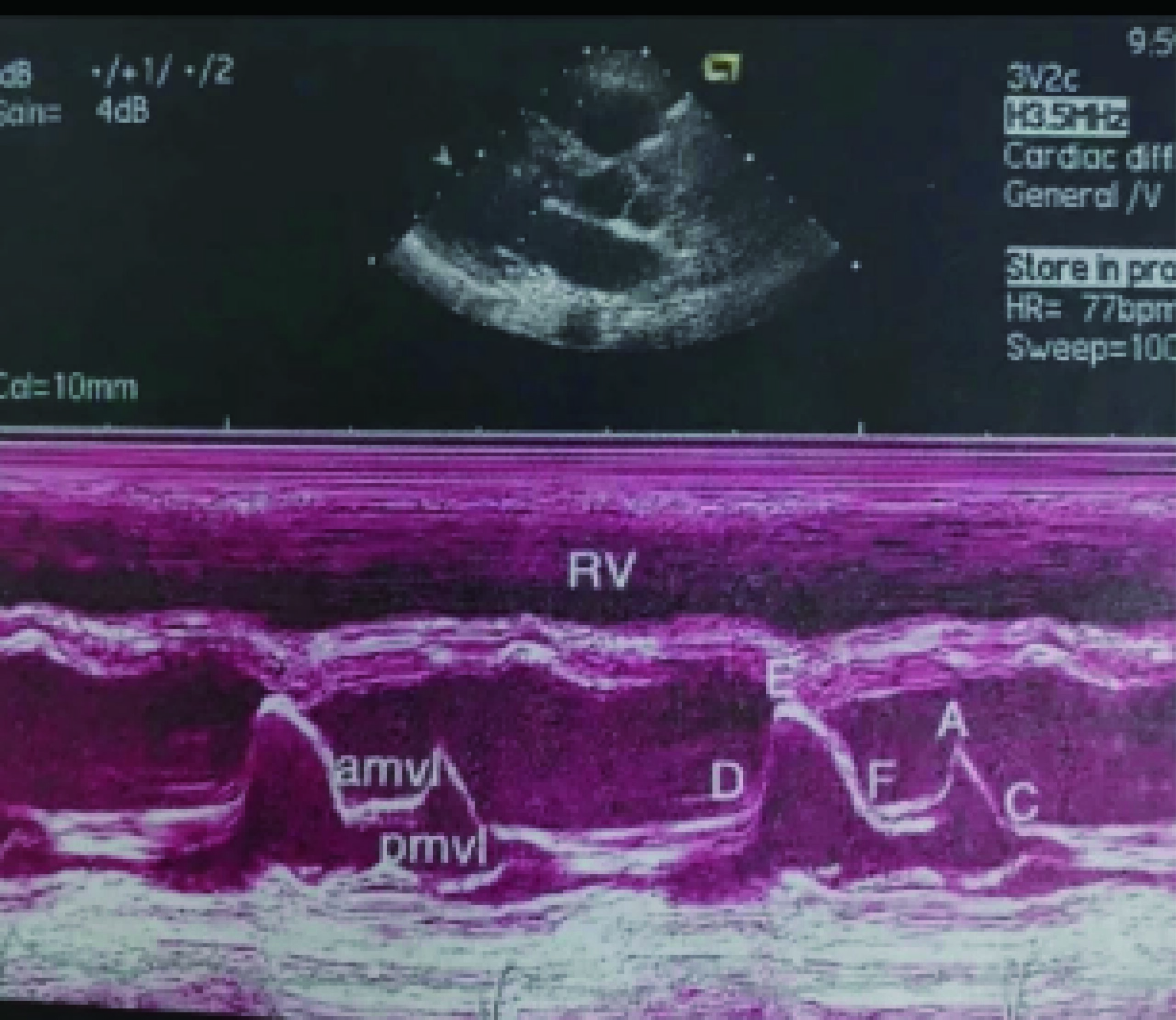
Figure 3
amv1 (anterior mitral valve leaflet)
Pmv1 (posterior mitral valve leaflet)
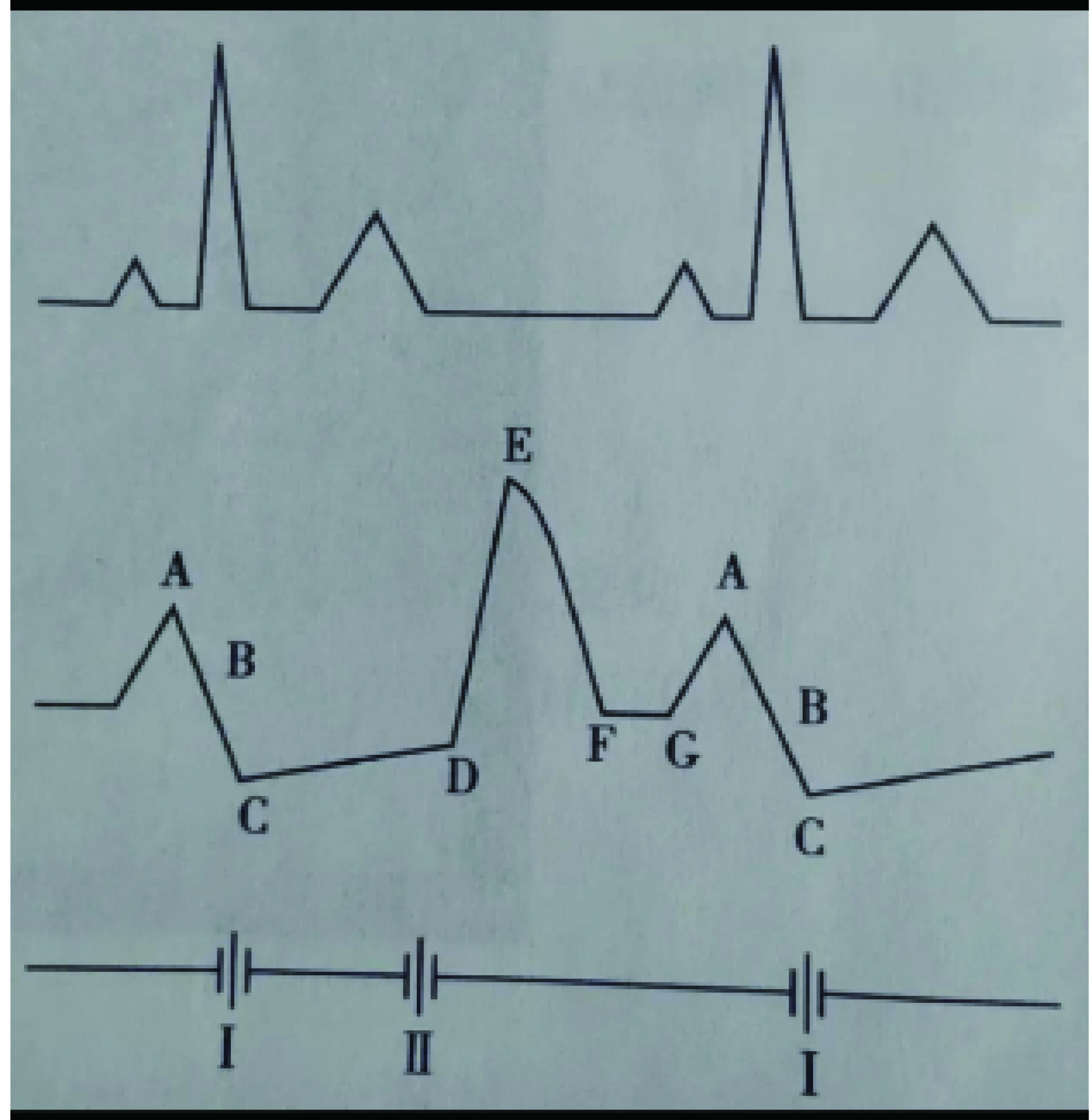
Figure 4
Points A, B, C, D, E, F
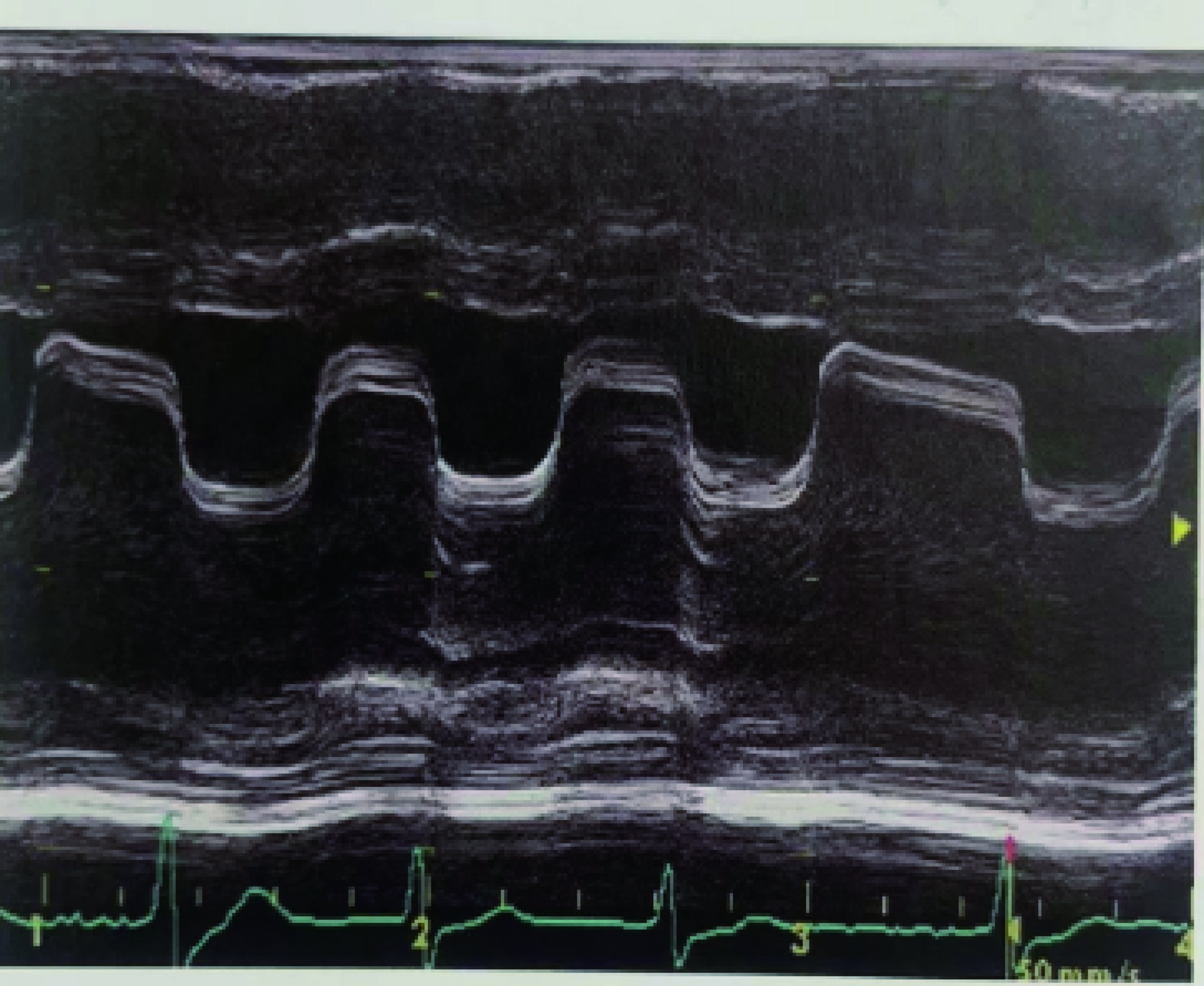
Figure 5
"Wall-like" curve in mitral stenosis
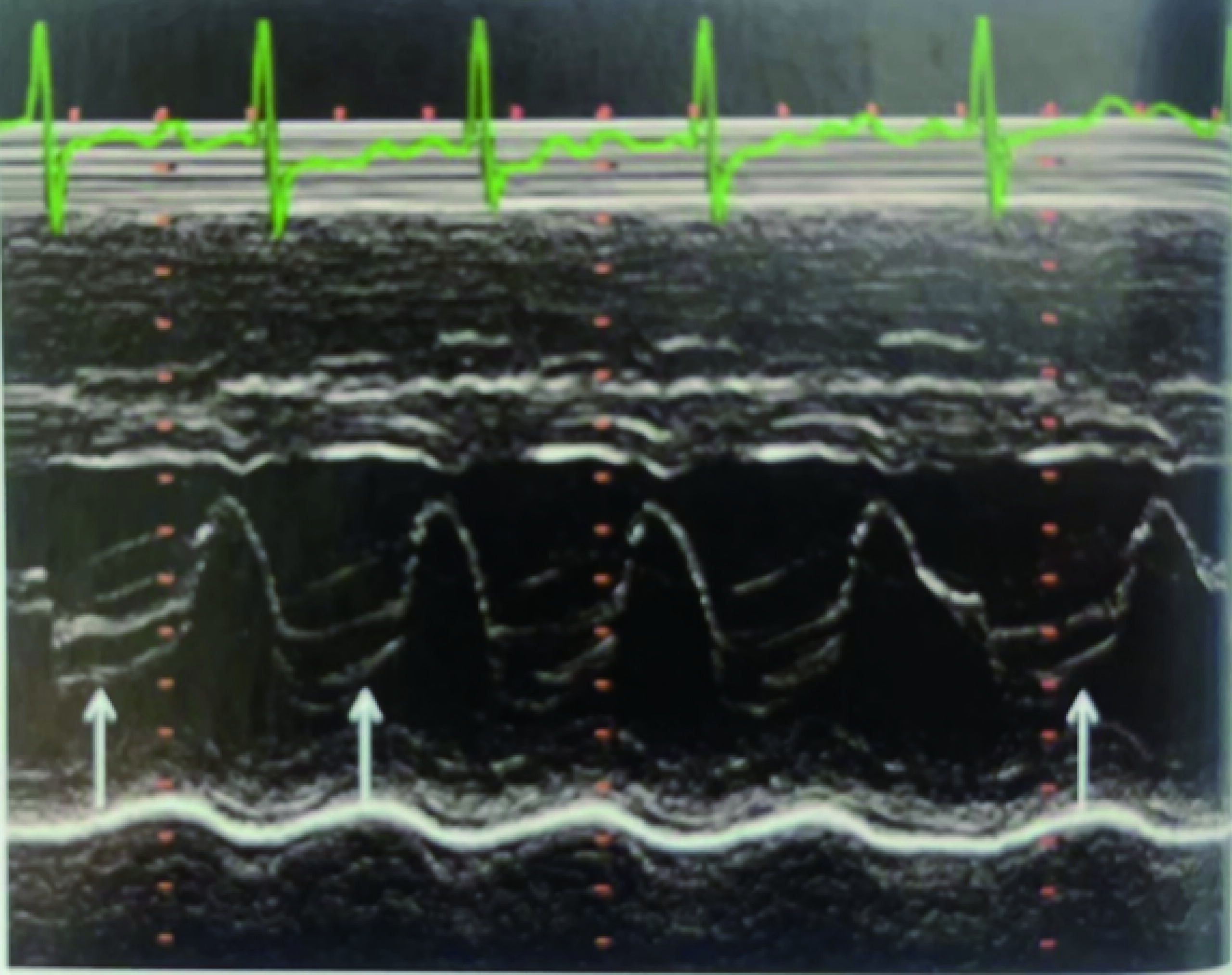
Figure 6
"Hammock-like" curve in mitral valve prolapse
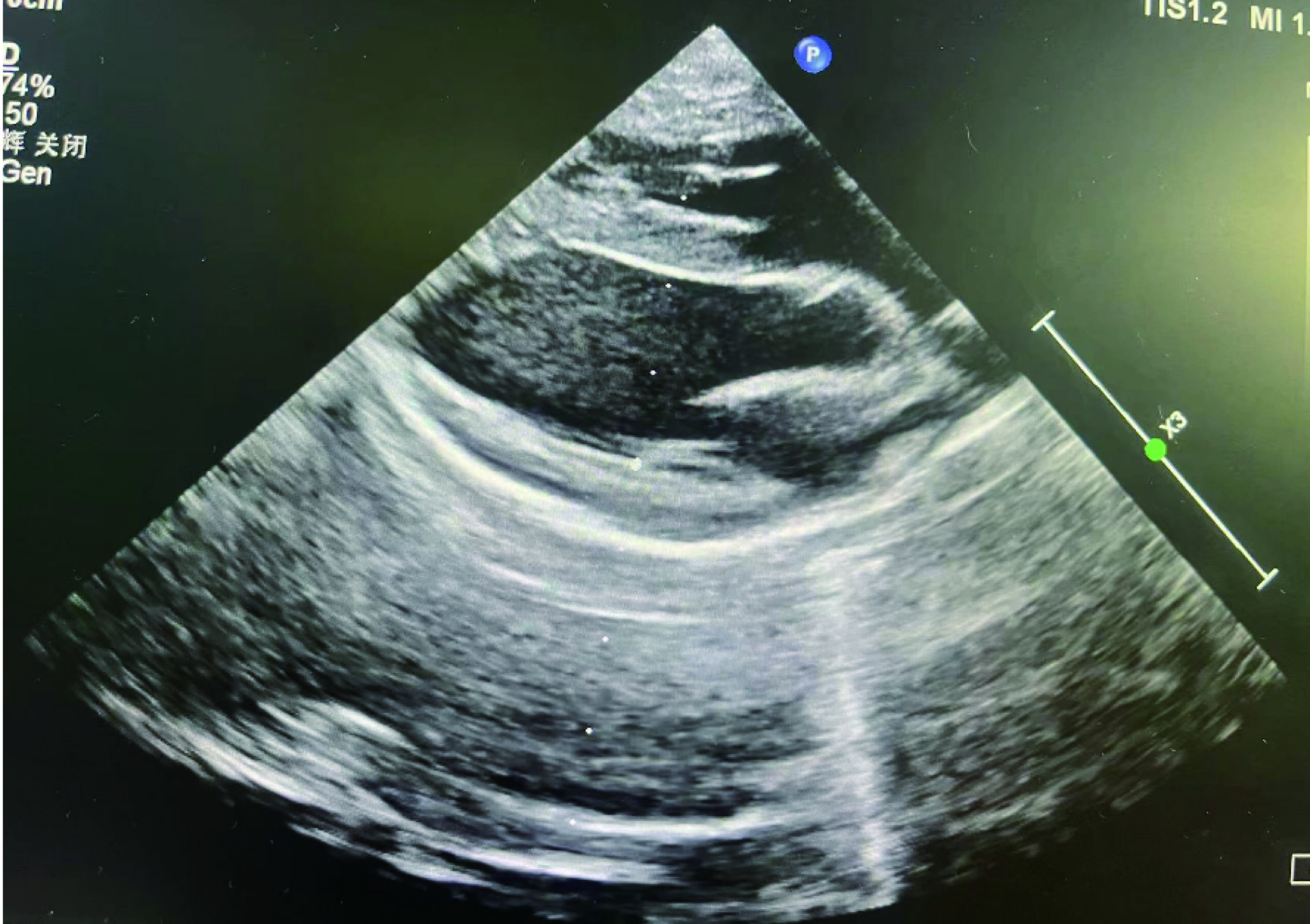
Figure 8
M-mode sampling line positioning at the chordae tendineae level (left ventricular long-axis view)